
Mid-Term Outcomes of Arthroscopically-Assisted Ligament Reconstruction | AC Joint

Mid-Term Outcomes of Arthroscopically-Assisted Anatomic Coracoclavicular Ligament Reconstruction Using Tendon Allograft for High-Grade Acromioclavicular Joint Dislocations
** Please Note: This article was among the five finalists in 2 categories for the following:
- Arthroscopy Journal Award for Clinical Research Excellence AND
- Arthroscopy Journal Award for Resident/Fellow Research Excellence
Authors:
Philip C. Nolte, M.D., M.A., Joseph J. Ruzbarsky, M.D., Bryant P. Elrick, M.Sc., Thomas Woolson, B.S., Kaare S. Midtgaard, M.D., Peter J. Millett, M.D., M.Sc.
Abstract:
Purpose
Methods
Results
Conclusion
Level of Evidence
AC Separation Treatment
AC Separation Treatment Overview
The collarbone (clavicle) attaches to the roof of the shoulder (acromion) in a joint known as the acromioclavicular (AC) joint. This area of the shoulder is easily defined because it is the bump that you can feel on the top of the shoulder. The collarbone is also stabilized in this area by ligaments called the coracoclavicular ligaments. These ligaments attach the collarbone to the front of the shoulder blade (scapula). Direct trauma to this shoulder area from a fall or a direct hit during sports activities can damage the connections and lead to an injury where the collarbone and roof of the shoulder are no longer sitting next to each other. This is often referred to as an AC separation and leads to elevation of the collarbone that can be felt at the top of the shoulder. When an AC separation is not healing with conservative treatment options, a surgical AC separation treatment may be recommended by Dr. Peter Millett.
An AC separation occurs when the clavicle and acromion are no longer aligned correctly. In mild AC separations, the injury may be treated by conservative measures such as rest, sling use and a short physical therapy rehabilitation program. If there is continued pain and limited function of the AC joint because the AC separation is not healing, or an uncomfortable amount of pain associated with overhead activities (such as throwing, lifting and reaching) is present, a minimally invasive AC separation treatment known as arthroscopic shoulder surgery for AC repair can be performed by Dr. Millett.
An AC separation treatment is an exciting new technique that allows for the repair of acute or chronic AC separations not healing with conservative measures. The surgery is performed on an out-patient basis, and full range of motion is quickly re-established within days of the procedure. During this out-patient procedure, also called the “Mumford” procedure, the end of the collarbone is removed through several tiny incisions. Once inside the shoulder, the clavicle is repaired and fixed back to its proper position. This technique is very successful for painful joints (weightlifters, arthritis, or minor separation).
Following a surgical AC separation treatment, patients will start shoulder motion under the direction of Dr. Millett and his team. Patients will be asked to wear a sling to protect the shoulder joint for several weeks following surgery. Eventually, after the ligaments heal, patients will be allowed to progressively strengthen the shoulder and discard the sling. Many patients can expect to return to sporting activities usually around 3 to 4 months following surgery.
For more information on AC separations, or to learn more about AC separation treatment, please contact the office of Dr. Peter Millett.
AC Joint
An Overview of the AC Joint
The acromioclavicular joint, also known as the AC joint, is located where the clavicle (collarbone) meets the highest point of the acromion (shoulder blade). The shoulder AC joint is small and has a limited range of motion, unlike the shoulder joint. The AC joint is a critical structure within the shoulder since it is the main connection between the arm and the axial skeleton. Dr. Peter Millett, orthopedic shoulder specialist, is well-trained and highly experienced at treating orthopedic injuries and sports injuries associated with the acromioclavicular joint.
CLICK IMAGE TO ENLARGE
AC Joint Function
The AC joint is classified as a synovial joint. Located where the collarbone meets the shoulder blade, the shoulder AC joint allows the arm to raise above the head. It also allows the transmission of forces from the upper arm to the rest of the skeleton. The joint itself does not have its own musculature, so movement is initiated elsewhere. For instance, when the arm is raised or rotated, the AC joint moves to accommodate the action.
AC Joint Anatomy
The acromioclavicular joint’s articular surfaces are lined with fibrocartilage, much like those of the sternoclavicular joint. The cavity of the AC joint is partially divided by an articular disc that is classified as a wedge of fibrocartilage suspended from the capsule’s upper portion.
The shoulder AC joint capsule is composed of a loose fibrous layer which encloses the two articular surfaces. As a synovial joint, the joint capsule is lined by a synovial membrane that releases synovial fluid into the joint cavity.
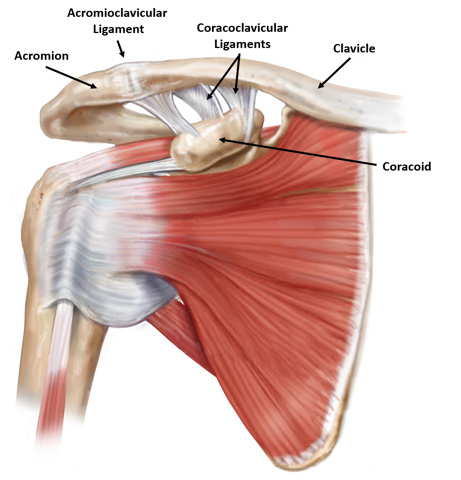
The acromioclavicular joint is stabilized by three ligaments and two sets of muscles. The acromioclavicular ligament runs horizontally from the shoulder blade to the collarbone. The two coracoclavicular ligaments connect the coracoid process, portion of the scapula, to the collarbone. The two sets of muscles responsible for assisting with the support of the AC joint include the trapezius muscle and deltoid muscle.
Injuries related to the AC joint are fairly common and often result from a hard fall or other trauma. Some examples of these injuries include:
Dr. Millett will perform a thorough physical examination to assess a patient’s shoulder AC joint injury, and then will discuss appropriate treatments that are available for patients from Vail, Aspen and the surrounding Denver, Colorado communities.
For additional resources on the AC joint, please contact the orthopedic practice of Dr. Peter Millett.
AC Joint Sprain
An Overview of an AC Joint Sprain
An AC joint sprain is a fairly common shoulder injury among active individuals. A shoulder sprain in the AC joint is typically caused by a direct blow to the “point” of the shoulder or a fall onto the shoulder joint. An AC joint sprain is characterized by the tearing of the connective tissue and ligaments of the acromioclavicular (AC) joint. Dr. Peter Millett, serving patients from Vail, Aspen and the surrounding Denver, Colorado communities, specializes in diagnosing and treating shoulder pain associated with a shoulder sprain in the AC joint.
The AC joint is responsible for connecting the shoulder blade to the clavicle. The joint allows for a small range of shoulder movement compared to the shoulder joint. When the AC joint is put under extreme stress during sports or work activity, it has the potential to tear. When a tear occurs, it is known as an AC joint sprain. A shoulder sprain in the AC joint can range from a small sprain, causing minimal shoulder pain, to a severe sprain causing extreme pain, instability and deformity.
What are the Symptoms of an AC Joint Sprain?
Many individuals who sustain an AC joint sprain will experience a sudden onset of shoulder pain located at the top of the shoulder joint. The pain may increase during certain activities such as overhead lifting, pushing and pulling movements and when moving the arm across the body. In a minor AC shoulder sprain, an individual may be able to perform daily activities with limited pain, swelling and stiffness. In more severe cases, a deformity may be visible from the tearing of the connective tissue holding the AC joint together.
How is an AC Joint Sprain Diagnosed?
In order to diagnosis a shoulder sprain of the AC joint, Dr. Millett will perform a thorough physical examination. He will ask questions regarding the patient’s medical history as well as what led to the injury. Dr. Millett will also move the affected shoulder to determine areas of shoulder pain and weakness. X-rays and an MRI may also be performed to determine the extent of the AC joint sprain and to rule out any other possible shoulder injuries.
How is an AC Joint Sprain Treated?
Active individuals can recover from an AC shoulder sprain in a few weeks without the need of surgical intervention. Dr. Millett typically begins with conservative treatment options to alleviate shoulder pain such as rest, activity modifications, shoulder immobilization, ice and a physical therapy program.
Dr. Millett may recommend surgical treatment if conservative treatments do not alleviate the symptoms. Surgery may also be recommended for athletes and workers that require a full recovery to perform necessary, everyday movements. There are numerous procedures designed to treat an AC joint sprain, including arthroscopic shoulder surgery for AC repair. Dr. Millett will explain the different treatment options to his patients and will suggest the best course of action.
For additional information on an AC joint sprain, or to learn more about treatment options shoulder pain and other shoulder conditions, please contact the office of Dr. Peter Millett.
AC Joint Separation
AC Joint Separation Overview
An AC joint separation is a common injury among physically active individuals. A separated shoulder is not truly an injury to the shoulder joint, but instead involves the acromioclavicular joint, otherwise known as the AC joint. In an AC separation injury, the clavicle (collarbone) separates from the scapula (shoulder blade), and is commonly caused by a fall directly on the shoulder or a direct blow. Dr. Peter Millett is a leading orthopedic shoulder specialist in the treatment of AC joint separations.
A separated shoulder is most commonly experienced when an individual falls directly on the “point” of the shoulder blade. The fall can be responsible for injuring the surrounding AC joint ligaments, the acromioclavicular ligament (AC) and the two coracoclavicular ligaments (CC), which stabilize the AC joint.

CLICK IMAGE TO ENLARGE
An AC separation injury can range from a mild separated shoulder to a complete tear of both the AC ligament and CC ligaments. Many physicians range the injuries on a Grade I-III scale.
What are the Symptoms of a Separated Shoulder?
An AC joint separation has a wide range of symptoms dependent on the grade of injury.
- Grade I: A slight stretch or partially torn AC ligament may cause joint tenderness, bruising and minor shoulder pain.
- Grade II: A completely torn AC ligament and intact CC ligaments may cause moderate to severe shoulder pain, swelling and a small bump on the top of the shoulder.
- Grade III: Completely torn AC ligament and CC ligaments may cause swelling, severe shoulder pain, shoulder deformity, and instability. Often a popping sound is heard at the time of injury.
CLICK IMAGE TO ENLARGE

CLICK IMAGE TO ENLARGE
CLICK IMAGE TO ENLARGE
CLICK IMAGE TO ENLARGE
How is an AC Joint Separation Diagnosed?
A separated shoulder is easy to diagnose when the injury causes deformity. When deformity is not present, a thorough physical examination must be performed to locate the area of pain and to compare the injured arm’s position to the uninjured arm. During the physical examination, Dr. Millett will gently feel the bones and soft tissues in the injured area, evaluate the range of motion and perform tests to locate specific areas of shoulder pain and weakness.

CLICK IMAGE TO ENLARGE
How is a Separated Shoulder Treated?
AC joint separation treatment depends on the injury grade. Many patients will experience a full recovery with non-operative treatment which includes rest, ice, shoulder immobilization, pain and anti-inflammatory medications, and physical therapy.
Surgery may be recommended by Dr. Millett if the AC separation is too severe or if non-operative treatment measures do not alleviate the separated shoulder symptoms. A variety of surgical measures may be used. The most common technique involves the reconstruction of the CC ligaments and performing a distal clavicle resection. During this procedure, Dr. Millett removes a tiny part of the collarbone, then transfers the AC ligament from the bottom of the shoulder blade to the end of the prepared collarbone, replacing the torn ligament. Dr. Millet can discuss the different surgical options individually, depending on the specific injury.
For additional information on an AC joint separation, or to learn more about treatment options for this shoulder condition, please contact Dr. Peter Millett.
AC Joint Separation Grading
AC Joint Grading System Overview
An acromioclavicular (AC) joint separation is the medical classification for the separation of the collarbone from the shoulder blade. An AC joint separation is a common injury in the active population and typically occurs from a hard fall or direct hit to the AC joint. AC joint separation grading helps physicians properly diagnosis and plan for proper treatment based on the extent of injury. The AC joint grading system includes a scale of six grades, and is determined by the level of separation found in the diagnostic x-ray and MRI. The most common AC separations are grade 1 through grade 3. Dr. Peter Millett specializes in diagnosing and treating AC joint injuries, helping patients return to the athletic activities they love.
AC Joint Separation Grading Scale
During an injury to the AC joint, soft tissues may become torn, leading to a varying amount of damage. An AC joint separation is graded by the extent of damage sustained to the ligaments. An AC joint separation grading scale includes:
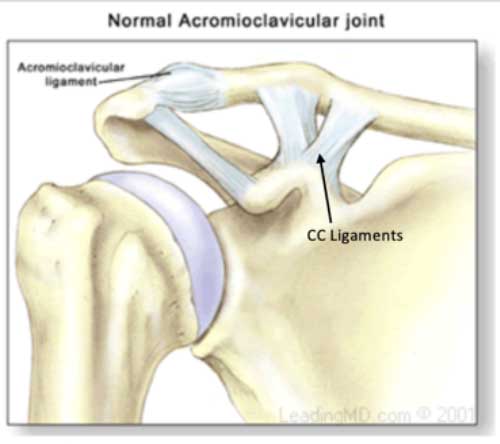
- Grade 1 – AC joint separation is a mild shoulder separation where the AC ligament is stretched or partly torn.
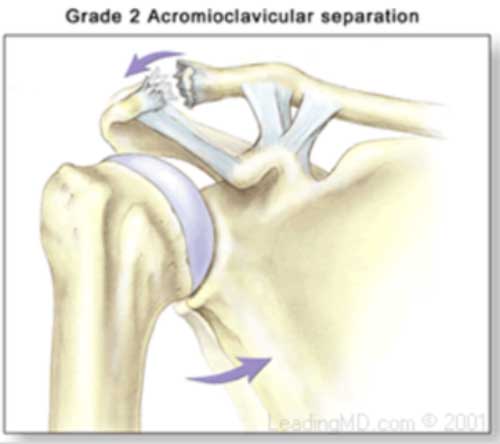
- Grade 2 – AC joint separation is a partial separation of the AC joint where the AC ligament is completely torn but the coracoclavicular (CC) ligaments are intact.
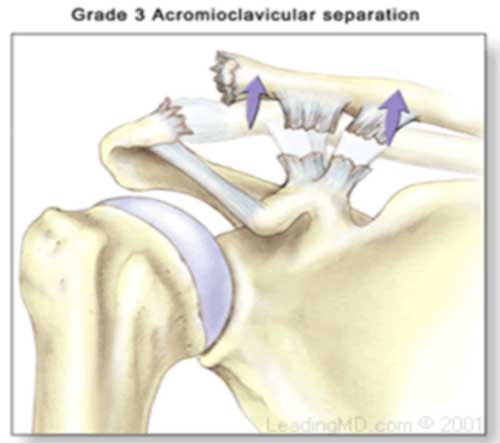
- Grade 3 – AC joint separation is a complete separation of the joint where the AC ligament and CC ligaments are completely torn, as well as the joint capsule.
- Grades 4, 5 and 6 – AC separations are extremely rare and occur when there is significant posterior movement of the clavicle (collar bone) in relation to the acromion (bony process on the shoulder blade).
What are the symptoms of AC joint separation?
The symptoms of an AC joint separation vary based on the extent of the injury. Treatment treatment options are dependent on the extent of the injury based on the AC joint grading system.
- Grade 1 – A grade 1 injury typically causes mild tenderness, bruising and minor pain.
- Grade 2 – A grade 2 injury typically causes moderate to severe pain, swelling and a small bump may be present on the top of the shoulder where the clavicle ends.
- Grade 3 – A grade 3 AC joint separation injury causes severe pain, swelling, instability and visible deformity.
AC Joint Separation Grading MRI and AC Joint Separation Grading X-Ray
In order to diagnose an AC joint injury and determine the injury level based on the AC joint grading system, Dr. Millett will perform a complete medical review and physical examination. He typically moves and feels the injured joint to get a better understanding of injury and to identify areas of pain and weakness. In many cases, Dr. Millett will perform an AC joint separation grading MRI and AC joint separation grading x-ray. Both diagnostic tests will help determine injury grade and an appropriate treatment plan.
The treatment of an AC separation depends on the injury grade. Grades 1-3 are commonly treated with non-operative measures such as rest, ice medication and arm stabilization in a sling.
Certain patients with a grade 3 AC joint separation will need a surgical treatment to fully recover. The surgical technique most commonly performed by Dr. Millett involves the reconstruction of the CC ligaments and the removal of a small piece of the clavicle at the shoulder. Using a screw or suture loop, he will stabilize the joint which allows for a full recovery in most patients.
For more resources on the AC joint separation grading scale, or to determine your grade of injury with an AC joint separation grading x-ray and MRI, please contact the orthopedic office of Dr. Peter Millett.
AC Fracture
AC Fracture Overview
Injuries to the acromioclavicular (AC) joint are among the most common shoulder injuries in the active population. The AC joint is located where the clavicle (collarbone) meets the highest point of the acromion (shoulder blade). An AC fracture is an injury that occurs when a break or crack becomes present in a bone in the AC joint area. A broken shoulder or fractured AC joint is often the result of a direct hit to the “point” of the shoulder or from a fall directly on the joint. Dr. Peter Millett, orthopedic shoulder specialist, is highly trained and experienced at treating a broken shoulder bone with both non-surgical and surgical options for patients in Vail, Aspen and the surrounding Denver, Colorado communities.
What are the symptoms of an AC fracture?
A broken shoulder bone in the AC joint area will cause a patient to experience shoulder pain, swelling, bruising and limited range of motion. Some patients may also have a visible deformity that is similar to a bump underneath the skin at the top of the shoulder.
How are AC Fractures Diagnosed?
Many cases of a broken shoulder in the AC joint area are diagnosed with an X-ray and a physical examination of the shoulder. If Dr. Millett suspects additional soft-tissue involvement he may request an MRI.
What is the treatment for an AC Fracture?
A broken shoulder bone in and around the AC joint is commonly placed in a sling and can be treated with more conservative measures such as rest, ice and activity modifications. Dr. Millett may recommend shoulder surgery if there is a moderate amount of bone displacement. This is done to bring the bones of the shoulder back into proper alignment so they can heal correctly. Surgery is also almost always recommended in patients who have experienced an open AC fracture which occurs when the broken bone has ruptured through the skin.
For additional information on an AC fracture, or to learn more about treatment options for a broken shoulder bone, please contact the practice of Dr. Peter Millett.
AC Arthritis
An Overview of AC Arthritis
Arthritis affects millions of Americans. AC arthritis, or osteoarthritis of the acromioclavicular joint, is quite common in middle-aged adults. This specific type of shoulder arthritis develops when the AC joint begins to deteriorate from loss of cartilage, causing AC joint pain and a limited range of motion in the shoulder. Dr. Peter Millett, orthopedic shoulder specialist, cares for a wide range of AC joint injuries, including AC shoulder arthritis.
As individuals age, cartilage in the shoulder area begins to deteriorate from overuse or normal wear and tear. Many individuals who experience cartilage loss will develop osteoarthritis. AC shoulder arthritis, much like other forms of osteoarthritis, can cause joint pain, inflammation and swelling.
Other causes of AC arthritis include an old injury to the AC joint, such as an AC joint separation, or repetitive overhead lifting. Athletes participating in contact sports are also at a higher risk of developing shoulder arthritis in the future if a hard fall or blunt hit to the shoulder area is sustained.
What are the symptoms of AC Arthritis?
One of the most common symptoms of AC shoulder arthritis is AC joint pain, or shoulder pain. Other common symptoms include tenderness at the top of the shoulder, swelling and limited range of motion.
How is AC Arthritis Diagnosed?
In order to properly diagnosis AC joint pain and the presence of AC arthritis, Dr. Millett will perform a thorough physical examination. He will examine the shoulder for tenderness over the AC joint and the level of pain experienced when the joint is compressed or in motion. X-rays and an MRI may also be performed to confirm the AC shoulder arthritis diagnosis.
How is AC Arthritis Treated?
In many cases, AC arthritis treatment will begin with conservative measures such as rest, ice, cortisone injections and medications. If conservative measures do not alleviate AC joint pain, Dr. Millett may recommend a surgical approach. The most common surgical procedure used to treat AC shoulder arthritis is resection arthroplasty. During this procedure, a small amount of bone from the end of the collarbone is removed. The removal of this area of bone leaves a space that gradually fills with scar tissue. The procedure is effective in fighting the painful symptoms of AC arthritis.
For additional resources on AC arthritis, please contact the orthopedic practice of Dr. Peter Millett.
AC Joint Research