

An Overview of a Distal Biceps Tear
Tears of the biceps tendon at the elbow is relatively uncommon.
The biceps is a muscle located in the front part of the upper arm that goes from the elbow to the shoulder. Tendons attach muscles to bones. Within this region of the upper arm, there are two groups of tendons associated with the biceps muscle. One group attaches the upper parts of the biceps to the shoulder blade (proximal, or upper biceps tendons), while the second group attaches the biceps to the elbow (distal, or lower biceps tendon).
The lower biceps tendon — the distal biceps tendon — can become injured from excessive loading or a violent force and can lead to tearing or ‘rupture’ of the tendon. Most often, this injury occurs among middle-aged men during heavy weight training workouts or in jobs where heavy lifting is involved. Corticosteroid medications and smoking are additional risk factors for this injury. A distal biceps tear can be very painful and most often is accompanied by a loud ‘pop’. This injury will cause pain and possibly discoloration under the skin, along with distortion of the normal contour of the skin as the muscle bunches up above the elbow.

Symptoms of a Distal Biceps Tear
Distal biceps tears and ruptures are somewhat uncommon, accounting for about three percent of all tendon ruptures. Once a distal (near the elbow) biceps tendon tear ruptures, symptoms will appear almost immediately. Those include:
- Intense pain followed by milder, throbbing pain
- Swelling of the biceps area
- Bruising of the biceps area
- Weakness in the arm, particularly with rotating the forearm (palm-up to palm-down)
- Inability to bend the elbow
- Change in the normal contour of the upper arm
Diagnosis of a Biceps Tear
Dr. Millett will perform a comprehensive physical exam that includes assessing range of motion, strength, and tenderness. If the tear is suspected in the elbow, Dr. Millett will ask you to rotate your forearm against resistance and compare the strength of this maneuver with the opposite side. Additionally, X-ray, Ultrasound, or MRI may be ordered.
Treatments for a Distal Biceps Tear
Non-Surgical
Treatment for torn biceps muscles varies. While nonsurgical treatment can be used, most active individuals who experience a distal biceps rupture will opt to have surgery in order to preserve full muscle strength. Non-surgical treatment for torn biceps muscles is best suited for those who have only a partial tear or those who do not participate in physically demanding upper-body activities. Non-surgical treatment consists of protecting the arm, resting the arm in a sling, physical therapy exercises, and managing pain with common over-the-counter medications for inflammation and pain.
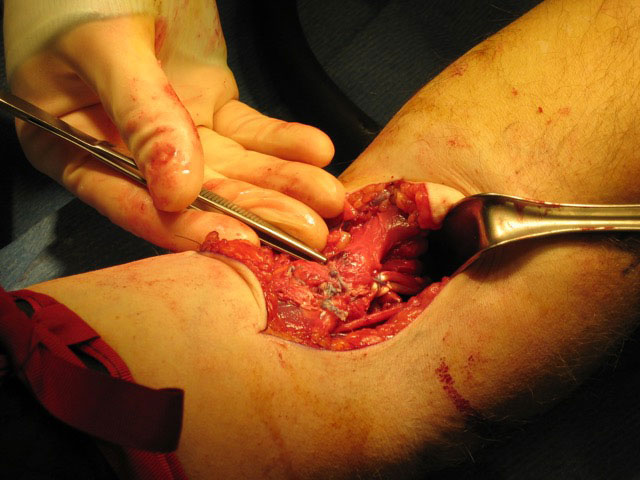
Surgical
If the biceps tendon tears completely, surgical repair can be a good option to restore function and to decrease pain. Dr. Millett uses a minimally invasive surgical technique to repair a distal biceps tendon tear. This is usually done right after the injury occurs and is done to reconnect the tendon to the correct location on the bone from which it has torn. For more chronic injuries, where the tendon has retracted or become severely scarred, a graft may be needed to reconstruct the torn tendon and connect it back to bone. Dr. Millett has recently written a comprehensive scientific review paper for the Journal of Bone and Joint Surgery on this topic and is highly experienced at repairing biceps injuries.

Have you experienced a distal biceps tear?
There are two ways to initiate a consultation with Dr. Millett:
You can provide current X-rays and/or MRIs for a clinical case review ($500).
You can schedule an office consultation with Dr. Millett.
For additional details on a distal biceps tear, please contact the office of Dr. Peter Millett.