
An Overview of Shoulder Instability and a Dislocated Shoulder
Shoulder instability is a condition that occurs when the muscles, tendons, bones, and ligaments that surround the shoulder do not work together to secure and maintain the ball (proximal humerus bone) within the socket (glenoid). When this happens, the shoulder is said to be unstable and the joint may either slide partially out of place which is known as a shoulder subluxation or it may slide completely out of place, which is called a shoulder dislocation. A dislocated shoulder is a common, yet frustrating shoulder injury. Dr. Peter Millett, orthopedic shoulder specialist, is experienced and skilled at helping patients from Vail, Aspen and the surrounding Denver, Colorado communities who have dislocated their shoulder or who have shoulder instability.
What causes shoulder instability?
When athletes suffer a blow directly to the shoulder, or when someone suffers trauma to the shoulder area either from a fall or an accident, shoulder instability can result. Instability can be a frustrating condition negatively affecting the patient until the condition is properly diagnosed and treated. Patients with shoulder instability will often complain about an uncomfortable sensation that their shoulder is about to “pop” or “slide” out of place. Sometimes it is more subtle however and pain may be the only manifestation of the condition. This condition usually affects the following distinct groups of patients:
- Patients who have had prior shoulder dislocations: Those patients who have had prior shoulder dislocations will often experience future dislocations, or recurrent instability. Age does play a crucial role in recurrent dislocations. When younger patients (35 years of age or younger) sustain a traumatic dislocation (from an injury), shoulder instability will follow in the vast majority of patients. In very young patients, those less than 20, the risk of suffering a second dislocation is almost 100 percent! On the other hand, older people (40 years of age and older) who experiences a traumatic dislocation will only have a 10% chance of developing chronic instability in future years, but they have an increasing risk of tearing the rotator cuff when the shoulder dislocates and that injury may need treatment in addition to the dislocation.
- Athletes: Athletes who participate in overhead activities such as basketball, swimming, gymnastics, and tennis may have continuing symptoms of a loose shoulder or experience multi-directional instability (slipping or dislocating in more than one direction). This is a condition that develops from loose ligaments and a stretched shoulder capsule. While a complete dislocation may not occur, it causes pain, weakness, and diminished function which may prevent athletes from participating in sports.
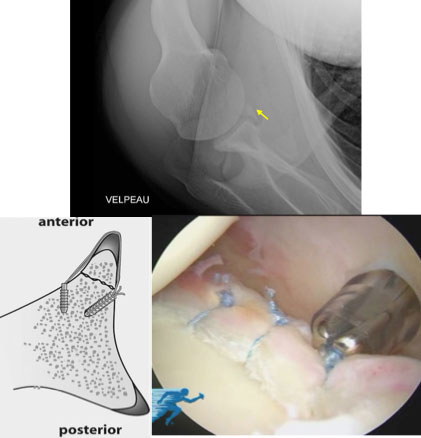
(Click to Enlarge) Top image is an x-ray demonstrating fracture of the anteroinferior glenoid rim (bony Bankart lesion: yellow arrow). Bottom left image illustrates the “bony Bankart bridge” technique. The bottom right arthroscopic image shows the final “bony Bankart bridge” repair.
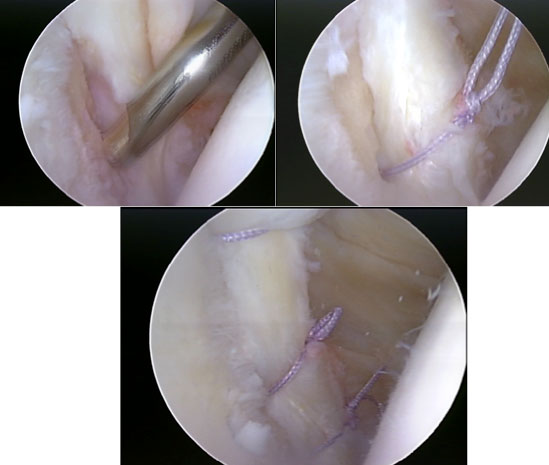
(Click to Enlarge) Top left arthroscopic image shows as Bankart lesion (tearing of the anteroinferior labrum). The top right arthroscopic image shows the tear being reduced with the first suture anchor. The bottom image shows the final repair of the Bankart lesion.

(Click to Enlarge) Postoperative x-ray image showing a glenohumeral fusion that was performed in a patient with intractable instability (repeated dislocations even after multiple stabilization procedures).
What are the symptoms of a dislocated shoulder and shoulder instability?
The symptoms associated with shoulder instability and shoulder dislocations include:
- Extreme pain in the shoulder region
- Apprehension (fear that the shoulder will come out)
- Restricted motion
- Popping or a sliding sensation
- Unusual shoulder position—for example, the shoulder may hang down and forward and appear “limp”
When a shoulder dislocation occurs, some individuals are experienced and might be able to “pop” their shoulder back into place (called a reduction). This is a very painful situation and attempting to reduce the shoulder should not be attempted. Many times a visit to the ER will be required to return the dislocated arm back to its socket.
Once a shoulder reduction has been performed, Dr. Millett will be able to determine the exact cause of the shoulder instability and the risk of recurrent dislocations with a physical examination and routine X-rays. Some times the X-ray might show a “bony Bankart” which is a fracture of the front, lower portion of the shoulder socket that occurs after a dislocation. This fracture—which is the most common cause of recurrent instability for young adults after an injury—indicates that the ligaments in the front of the shoulder are no longer attached to the glenoid. Another common finding is a Hill Sachs fracture, which is an indentation or impression fracture on the ball of the upper arm (proximal humerus) that occurs when it impacts the socket during the dislocation. These findings are frequently only part of the problem and additional tests such as an MRI are usually required to fully determine the extent of the damage.
What is the treatment for a dislocated shoulder?
Non-Surgical
Often times, patients who suffer from shoulder instability and shoulder dislocations can begin a structured physical therapy rehabilitation program using exercises to help strengthen the shoulder joint. Physical therapy with ongoing strengthening exercises will often help maintain the shoulder in proper position. Athletes typically benefit greatly from physical therapy for shoulder instability. Cortisone injections and anti-inflammatory medications are also used to help treat the condition and minimize pain.
Surgical
There are surgical options for shoulder instability if physical therapy is not an option, or if it fails to reduce pain and continued dislocations. Depending on the cause of the instability, arthroscopic surgery is the most preferred option. Dr. Millett also performs open treatment for instability.
Bankart-Capsulolabral Reconstruction
Bankart-type capsulolabral repair surgery is the most common surgery performed on patients with chronic instability who opt to have surgery. This procedure can be as an open procedure but Dr. Millett usually performs it arthroscopically (which is the preferred method). This is among the most frequent types of surgery that Dr. Millett performs. If the shoulder instability is chronic and is in the setting of ‘end-stage’ instability, then there are options such as a bone grafting procedure and soft tissue grafting procedure which can be used to restore stability to the shoulder joint. Capsulolabral reconstruction is one technique that Dr. Millett has helped develop. This is a technique in which a transplanted tendon (from another part of the body or from a cadaver) is used to make new ligaments (capsule) and cartilage (labrum), which then act to prevent dislocation and stabilize the chronically unstable shoulder.
For more information on shoulder instability, or to discuss treatment options for a dislocated shoulder, please contact the office of Dr. Peter Millett, serving patients in Vail, Aspen and the surrounding Denver, Colorado communities.
Related Articles
What Treatment Options Exist for Shoulder Instability?
Does My Son Need Surgery for a Dislocated Shoulder?
I Dislocated my Shoulder and have Ongoing Shoulder Instability. Why?